Pre-cancerous Lesions of the Pancreas (Overview)
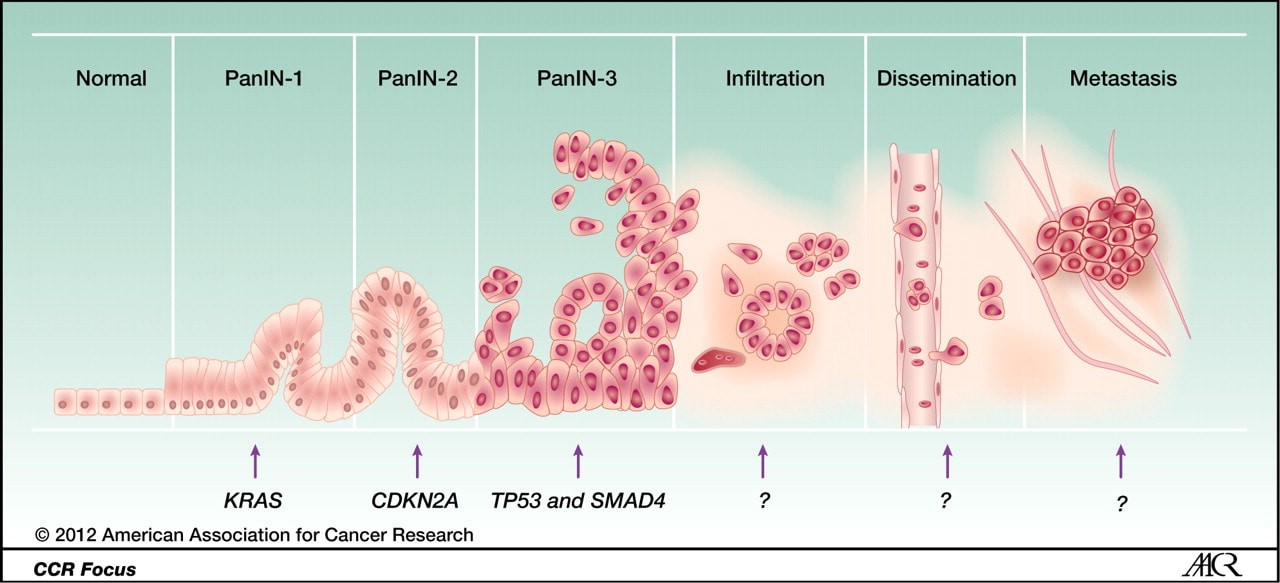
Christine A. Iacobuzio-Donahue, Victor E. Velculescu, Christopher L. Wolfgang and Ralph H. Hruban. Genetic Basis of Pancreas Cancer Development and Progression: Insights from Whole-Exome and Whole-Genome Sequencing. Clin Cancer. 2012.
